
The Jane Goodall of neurosurgery

“Be there by 5:30. If you make it at 5:31, you’re already late,” advised the resident I talked to the night before my neurosurgery elective in August. I woke up at 4 a.m., before the summer sun was up. One heaping spoonful of instant coffee later, I was on the 30-minute drive from the suburbs to the main hospital in downtown Detroit.
Six neurosurgery residents and three rotating medical students gathered under harsh fluorescent lights in the neurosurgical intensive care unit (NICU). Countless, faceless neurosurgery residents have been a part of my life since I can remember. They would call our home phone to discuss patients with my father, a senior neurosurgery staff, day and night. Six of those faceless humans were in scrubs and face masks. The rolling computers — called WOWs because a patient had been personally offended by the previous acronym COWs (computers on wheels) — started squeaking away at 5:30 a.m. on the dot.
The NICU houses the sickest patients. Patients with brain bleeds and complicated tumors. William Halsted, a cocaine-addicted surgeon from Johns Hopkins, set up the first formal residency program and rounding as we know it in the U.S. today. We continue the grueling process without cocaine, but with enough energy drinks to perhaps equivalate. Energy drinks contain B6, a vitamin that can be toxic to the nervous system in high doses. One of my friends recounted a story of a resident who developed B6 toxicity from drinking too many energy drinks.
We continue the grueling process without cocaine, but with enough energy drinks to perhaps equivalate.
We finished rounding in the NICU and crowded together in the little workroom in the corner of the unit at 6 a.m. The overnight on-call resident signed off all the patients to the oncoming on-call resident under the watchful gaze of the two seventh-year chief residents. In addition to the NICU patients, the neurosurgeons have patients in almost every corner of the hospital: a step-down ICU floor; a general floor; consults from acute trauma, oncology, internal medicine and neurology. Sign-out is a serious ordeal. A bouncing knee and fallen pen are conspicuous enough to make you want to wince. My knee and pen bounced a few times.
Seven senior staff arrived at the little workroom at 7 a.m. and went over patients’ brain imaging with the residents. Each staff member has a resident assigned to their service for three-month blocks. After looking at imaging, they divided and rounded on their respective patients all over the hospital. The residents made it back to their working space on the general floor to sign out updates to the resident on call that day. Most of the operating rooms start by 8 a.m. and last all day.
The OR is its own little ice-box cold world tucked away on the fourth floor of the hospital. The doors open to a wide room where flat screens have 30 OR room numbers next to the names of attending staff and cases. They’re reminiscent of airport flight screens. Surgeons, anesthesiologists, residents, technicians, nurses and medical students covered in light blue scrubs from head to toe dot their way through this maze.
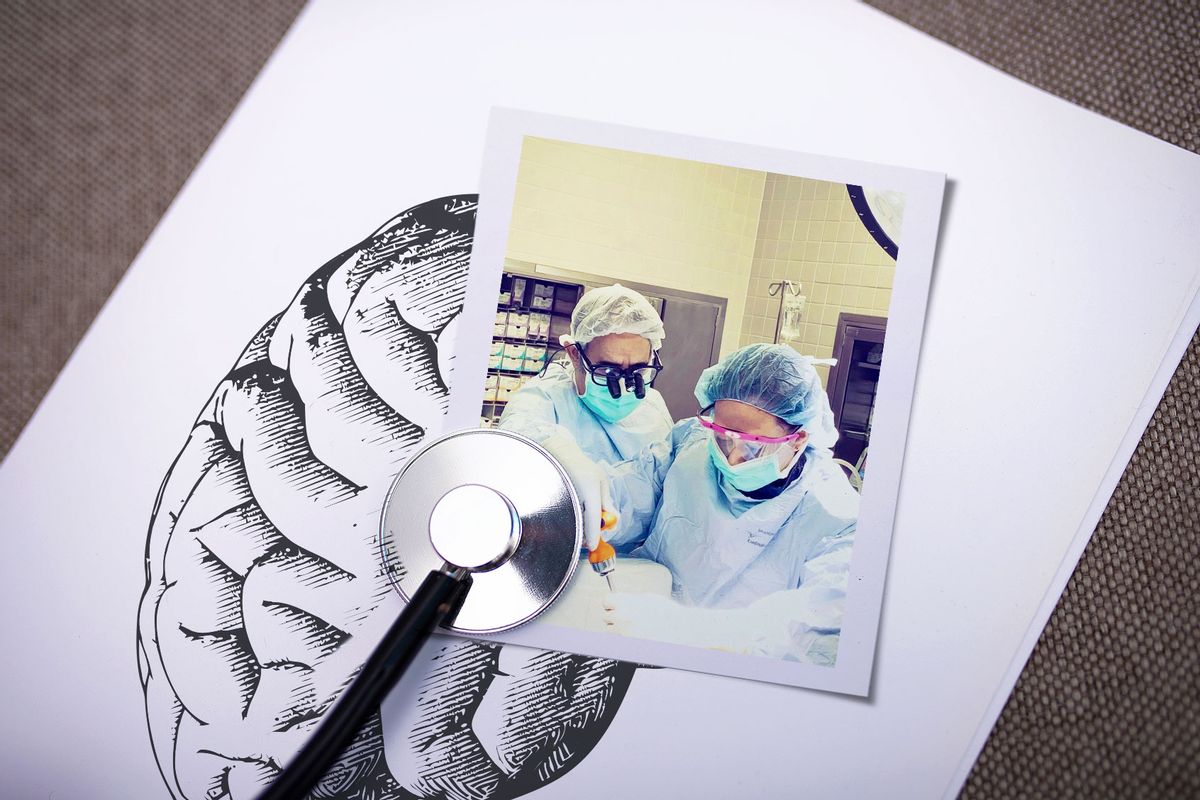
I am not sure how many females have historically had the chance to witness a living, pulsating human brain with their fathers.
Neurosurgery cases are famously long. The shortest case I have been in, from rolling the patient to the OR from their hospital bed and back to recovery, lasted at least five hours. One of the residents told me they stop eating and drinking during the day to avoid having to leave the OR and break sterility and scrub in again. I don’t have that kind of willpower or bladder capacity.
I am not sure how many females have historically had the chance to witness a living, pulsating human brain with their fathers. I watched mine perform a complicated skull-based surgery — the removal of a sphenoid meningioma. The meninges comprise three layers that surround the brain: pia, arachnoid and dura. Meningiomas, tumors of the meninges, are usually benign tumors that can require resection when they become symptomatic. There were too many people crowded around the patient’s head under a microscope, so I watched the camera screen from a little stool while wrapped in warm blankets.
It was a mental struggle being present during some of the cases. The fact that I couldn’t always stay focused while someone’s brain was open in front of me made me wonder at the ridiculousness of my own, at its frequent internal incoherence that drowns out the external world. I also wondered how the surgeons working with me were able to have such prolonged stretches of focused attention.
The last case of the day often ended at 7 or 8 p.m. Because this was an elective for me as a neurology resident, I often left much earlier, around 5 p.m. Even with the earlier time and without having to be on a 24-hour call every fourth day, the day was often long enough for me to regret my existence when I woke up at four in the morning the next day having to do it all over.
If you step into a hospital, you would be hard-pressed to describe how AI shall defeat death.
Henry Marsh—Mr. Henry Marsh, that is, because male surgeons in the UK are strangely prefixed with Mr. instead of Dr.—is a British neurosurgeon who wrote the astutely titled “Do No Harm,” a dictum of the Hippocratic Oath. The chapters in the book are named after mostly operable conditions: Pineocytoma, Aneurysm, Hemangioblastoma, Melodrama, Tic douloureux, Angor animi, Meningioma, Choroid plexus papilloma, Leucotomy, Trauma, Ependymoma, Glioblastoma, Infarct, Neurotemesis, Medulloblastoma, Pituitary adenoma, Empyema, Carcinoma, Akinetic mutism, Hubris, Photopsia, Astrocytoma, Tyrosine Kinase, Oligodendroglioma, Anesthesia dolorosa.
Marsh is British in his skepticism and honesty. He starts his book by wondering if his American colleagues realize the phrase “death is optional in America” was not meant to be literal. Yet, there are articles on how Artificial Intelligence may defeat death ad nauseam. If you step into a hospital, you would be hard-pressed to describe how AI shall defeat death. Death is so pathetically human that to counter it is deceptive. All this fantasy has accomplished is to annihilate the conversation about the concept of a good death and why it matters. It has annihilated the concept of a good life by the same token.
Mr. Marsh states there are only two good reasons to do medicine: for interesting anecdotes and to know the best medical care for yourself and your family. Anecdotes? We’re full of them. So full that our small lives have difficulty containing the square density they rapidly accumulate in our fragile hearts. One of the surgically complicated patients in the NICU recovers from a neurological standpoint. After we round on the patient one morning, I make a casual observation, to which one of the residents jokingly remarks, “You’re like the Jane Goodall of neurosurgery.” A week later the patient does well enough to be discharged from the NICU. Despite being on subcutaneous prophylactic anticoagulation, the patient unexpectedly dies of a sudden pulmonary embolism.
Read more
personal essays from physicians